סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
דו״ח מאומת
הסרטון מציג מידע מדויק ומגובה במחקרים מדעיים אמינים.
סיכום
כל הטענות שהוצגו נתמכות על ידי הספרות המדעית העדכנית ב-PubMed. הראיות מצביעות על קשר מובהק בין הרגלי תזונה (צריכת סיבים, החלפת שומן רווי בשומן מהצומח, הגבלת בשר מעובד וסוכר, ואכילת דגים) לבין שיפור במדדים קרדיווסקולריים ומטבוליים.
analytics ניתוח טענות מבוסס ראיות
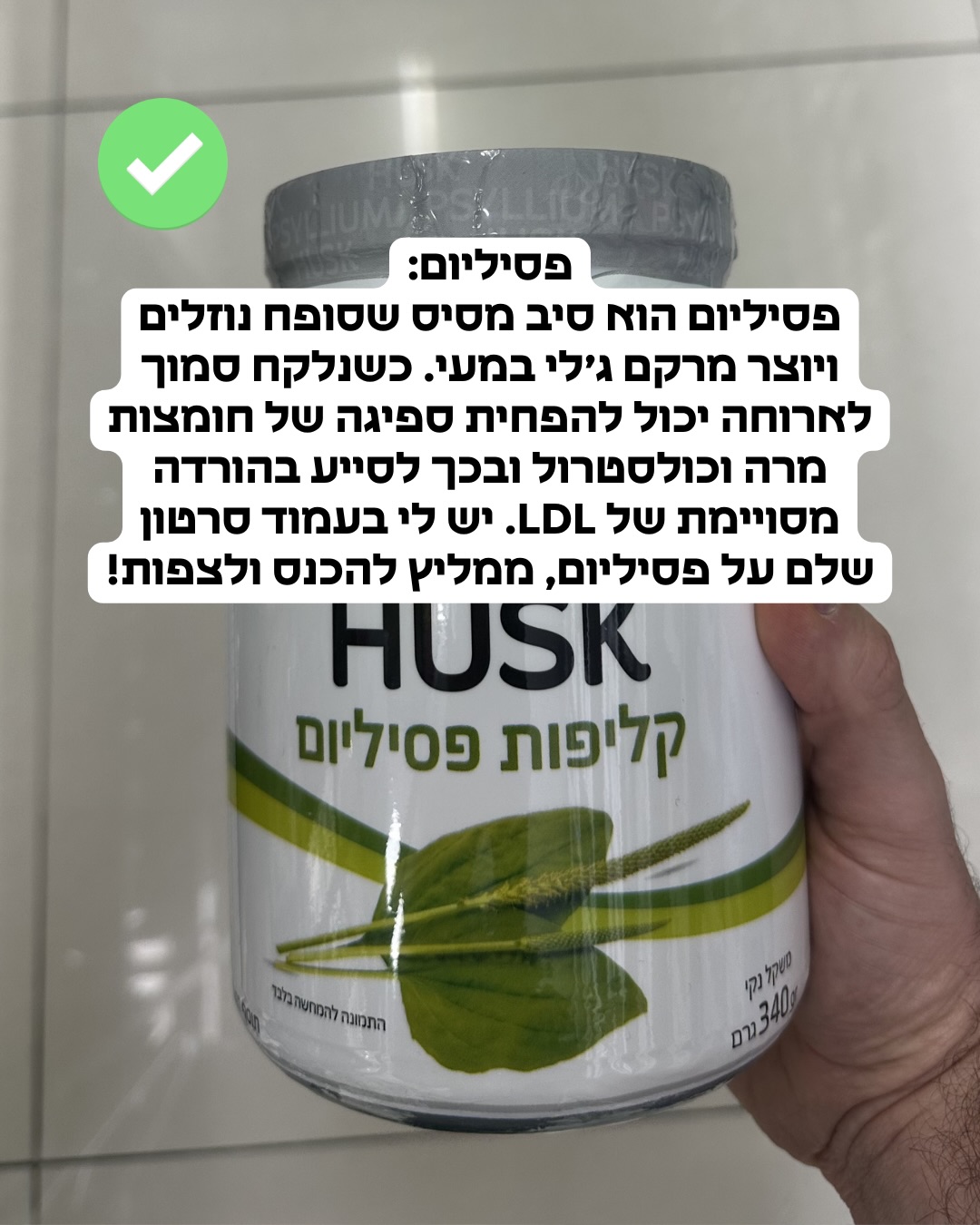
"צריכת סיבים מסיסים, כגון בטא-גלוקן הנמצא בשיבולת שועל ובגריסים או בתוספי פסיליום, מסייעת בהפחתת ספיגת הכולסטרול במעי ובהורדת רמות ה-LDL."
מסקנת הבדיקה:
מחקרים קליניים מבוקרים מאשרים כי סיבים מסיסים, כולל בטא-גלוקן ופסיליום, מסייעים בהורדת רמות ה-LDL בדם. המנגנון כולל יצירת ג'ל במעי המפחית את ספיגת הכולסטרול. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Effects of soluble dietary fiber on low-density lipoprotein cholesterol and coronary heart disease risk.
Strong epidemiologic and experimental data suggest that increasing dietary fiber may help to lower low-density lipoprotein cholesterol (LDL-C) and decrease the risk of coronary heart disease. Recent studies have highlighted the role of dietary fiber, particularly water-soluble varieties, in decreasing the risk of cardiovascular disease. Several types of soluble fiber, including psyllium, beta-glucan, pectin, and guar gum, have been shown to decrease LDL-C in well-controlled intervention studies, whereas the soluble fiber content of legumes and vegetables has also been shown to decrease LDL-C. Current investigations continue to explore this area in depth and examine potential synergies between dietary fiber and other phytochemicals that may lower cholesterol. These studies, along with recent analyses of ongoing prospective cohort studies, have provided new insights into the probable protective role of dietary fiber in the development of coronary heart disease and other cardiovascular diseases.…
PMID: 18937894
-
link
Water-soluble dietary fibers and cardiovascular disease.
One well-established way to reduce the risk of developing cardiovascular disease (CVD) is to lower serum LDL cholesterol levels by reducing saturated fat intake. However, the importance of other dietary approaches, such as increasing the intake of water-soluble dietary fibers is increasingly recognized. Well-controlled intervention studies have now shown that four major water-soluble fiber types-beta-glucan, psyllium, pectin and guar gum-effectively lower serum LDL cholesterol concentrations, without affecting HDL cholesterol or triacylglycerol concentrations. It is estimated that for each additional gram of water-soluble fiber in the diet serum total and LDL cholesterol concentrations decrease by -0.028 mmol/L and -0.029 mmol/L, respectively. Despite large differences in molecular structure, no major differences existed between the different types of water-soluble fiber, suggesting a common underlying mechanism. In this respect, it is most likely that water-soluble fibers lower the (re)absorption of in particular bile acids. As a result hepatic conversion of cholesterol into bile acids increases, which will ultimately lead to increased LDL uptake by the liver. Additionally, epidemiological studies suggest that a diet high in water-soluble fiber is inversely associated with the risk of CVD. These findings underlie current dietary recommendations to increase water-soluble fiber intake.…
PMID: 18302966
-
link
Soluble fiber intake at a dose approved by the US Food and Drug Administration for a claim of health benefits: serum lipid risk factors for cardiovascular disease assessed in a randomized controlled crossover trial.
The US Food and Drug Administration (FDA) approved health claims for 2 dietary fibers, beta-glucan (0.75 g/serving) and psyllium (1.78 g/serving), on the assumption that 4 servings/d would reduce cardiovascular disease risk. We assessed the efficacy of this dose of fibers in reducing serum lipid risk factors for cardiovascular disease. Sixty-eight hyperlipidemic adults consumed a test (high-fiber) and a control low-fat (25% of energy), low-cholesterol (<150 mg/d) diet for 1 mo each in a randomized crossover study. The high-fiber diet included 4 servings/d of foods containing beta-glucan or psyllium that delivered 8 g/d more soluble fiber than did similar, unsupplemented foods in the control diet. Fasting blood samples and blood pressure readings were obtained at baseline and weeks 2 and 4, and the subjects' weight was monitored weekly. Compared with the control diet, the high-fiber diet reduced total cholesterol (2.1 +/- 0.7%; P = 0.003), total:HDL cholesterol (2.9 +/- 0.8%; P = 0.001), LDL:HDL cholesterol (2.4 +/- 1.0%; P = 0.015), and apolipoprotein B:A-I (1.4 +/- 0.8%; P = 0.076). Applying the Framingham cardiovascular disease risk equation to the data confirmed a reduction in risk of 4.2 +/- 1.4% (P = 0.003). Small reductions in blood pressure were found after both diets. The subjects reported no significant differences in palatability or gastrointestinal symptoms between the diets. The reduction in serum lipid risk factors for cardiovascular disease supports the FDA's approval of a health claim for a dietary fiber intake of 4 servings/d. Although relatively small in terms of patient treatment, the reduction in cardiovascular disease risk is likely to be significant on a population basis.…
PMID: 11976156
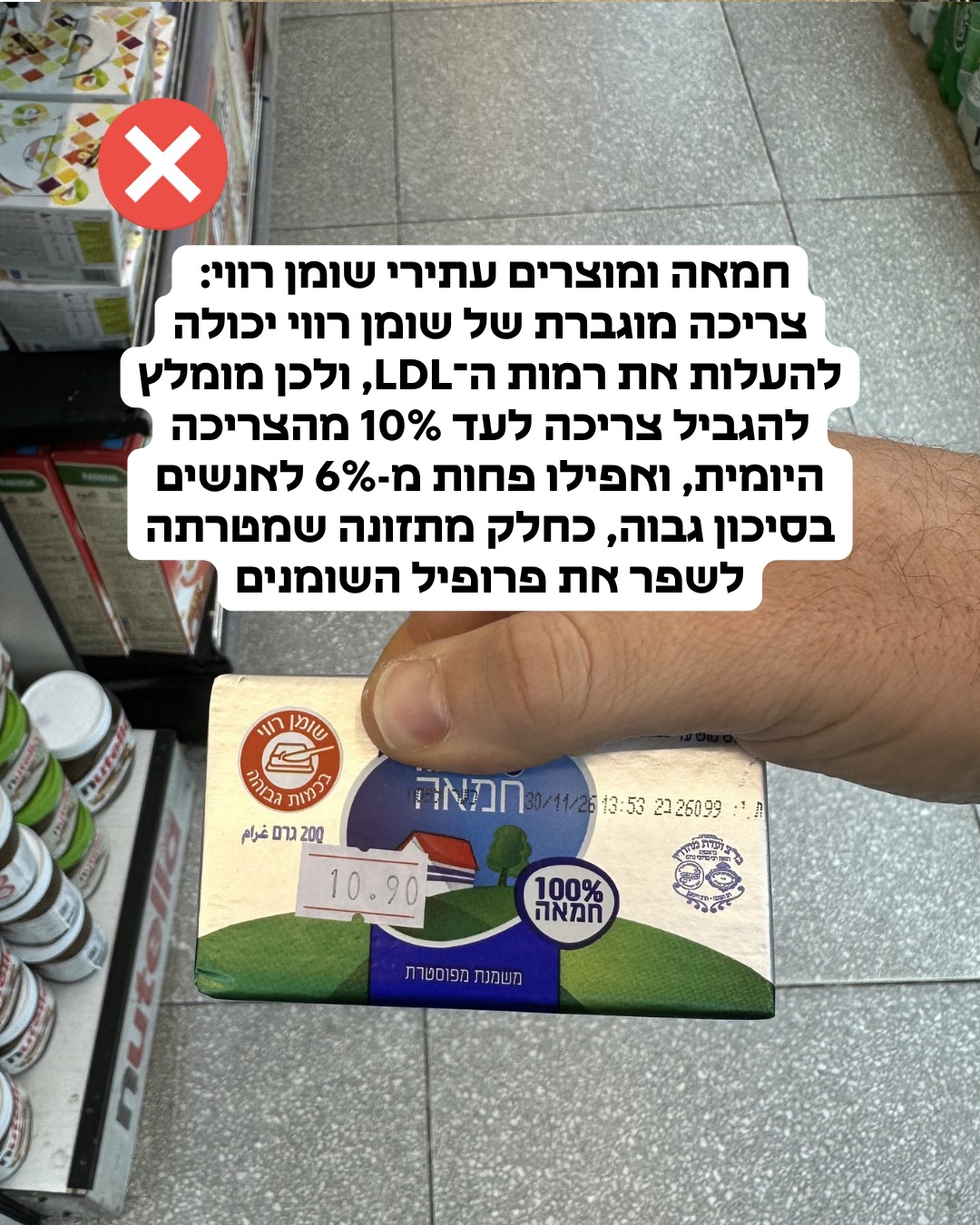
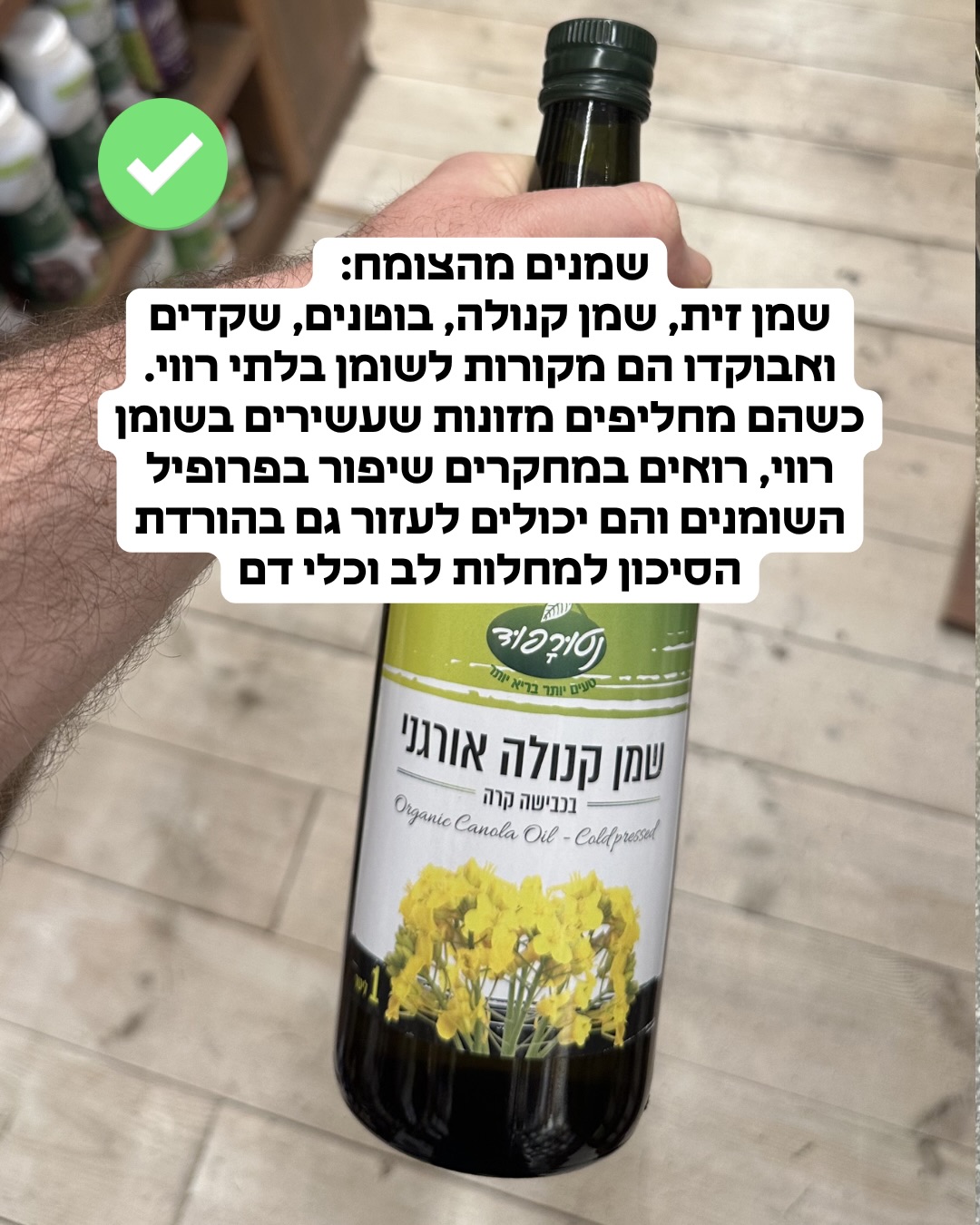
"צריכה מוגברת של שומן רווי (כמו בחמאה) עלולה להעלות את רמות ה-LDL, בעוד החלפתם בשומנים מהצומח (כמו שמן זית או קנולה) עשויה לשפר את פרופיל השומנים בדם."
מסקנת הבדיקה:
הספרות המדעית תומכת בכך שצריכת שומן רווי מעלה את רמות ה-LDL, בעוד החלפתו בשומנים בלתי רוויים מהצומח משפרת את פרופיל השומנים ומפחיתה סיכונים קרדיווסקולריים. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Ultra-processed Plant Foods: Are They Worse than their Unprocessed Animal-Based Counterparts?
This review aims to compare the impact of unprocessed animal foods with ultra-processed plant-based alternatives, particularly plant-based milks, plant-based meat analogs, and margarine, on cardiometabolic risk factors, chronic diseases, and mortality. The ultra-processed food category is highly heterogeneous, encompassing products with varying ingredients and nutrient profiles. Plant-based milks, plant-based meat analogs, and margarine, typically classified as ultra-processed foods, differ markedly from their unprocessed animal-based counterparts: they do not contain cholesterol or heme iron, have lower concentrations of saturated fat, sulfur, and branched-chain amino acids, and provide dietary fiber, which is absent in animal-based foods. Replacing dairy milk with soymilk have been shown to reduce total cholesterol (TC), LDL cholesterol (LDL-C), and C-reactive protein (CRP), and is associated with a lower risk of breast cancer. Compared to unprocessed animal-based products, plant-based meat analogs are associated with reductions in TC, LDL-C, body weight, plasma ammonia, and trimethylamine oxide (TMAO). Substituting butter with soft margarine reduces TC and LDL-C, and is associated with a lower risk of cardiovascular events and mortality. While ultra-processed plant-based foods are less healthy than whole plant foods, they may offer better cardiometabolic outcomes than unprocessed animal-based products. As transitional tools, products such as plant-based milks, meat analogs, and margarine may facilitate dietary shifts. Public health guidance should reflect these nuances to support realistic, health-promoting transitions.…
PMID: 41129036
-
link
Retrospective analysis of dietary fat quality and cardiovascular disease risk markers in middle-aged adults.
<h4>Background</h4>The quality of fat in food affects the cardiovascular system by means of inflammatory and lipid pathways.<h4>Objective</h4>To assess the relationship among middle-aged persons' cardiovascular disease (CVD) risk indicators and the composition of their dietary fat.<h4>Methodology</h4>Two hundred adults (aged 40-65) from the Henan Provincial Chest Hospital's databases were incorporated in this retrospective, hospital-based observational investigation. Dietary consumption information was taken from food frequency questionnaires that had been filled out and were kept in medical records. Employing the unsaturated-to-saturated fatty acid proportion (UFA:SFA), dietary fat composition was measured and subjects were separated into tertiles. Anthropometric variables, lipid levels (total cholesterol, LDL-C, HDL-C), and inflammation levels (hs-CRP) were obtained from pre-existing laboratory and hospital records.<h4>Results</h4>In comparison to the lowest tertile, the highest UFA:SFA tertile had greater HDL-C (+8.29 mg/dL, <i>d</i> = 1.54), decreased TC (-30.33 mg/dL, <i>d</i> = 2.86), LDL-C (-24.73 mg/dL, <i>d</i> = 2.67), and hs-CRP (-1.28 mg/L, <i>d</i> = 2.53; all <i>p</i> < 0.001).<h4>Conclusion</h4>Better lipid and inflammatory levels were associated with higher dietary fat quality, highlighting the significance of substituting unsaturated fats for saturated fats as a CVD prevention measure. However, prospective or interventional research are required to investigate causal effects, as these results are observational and demonstrate association rather than causality.…
PMID: 41311796
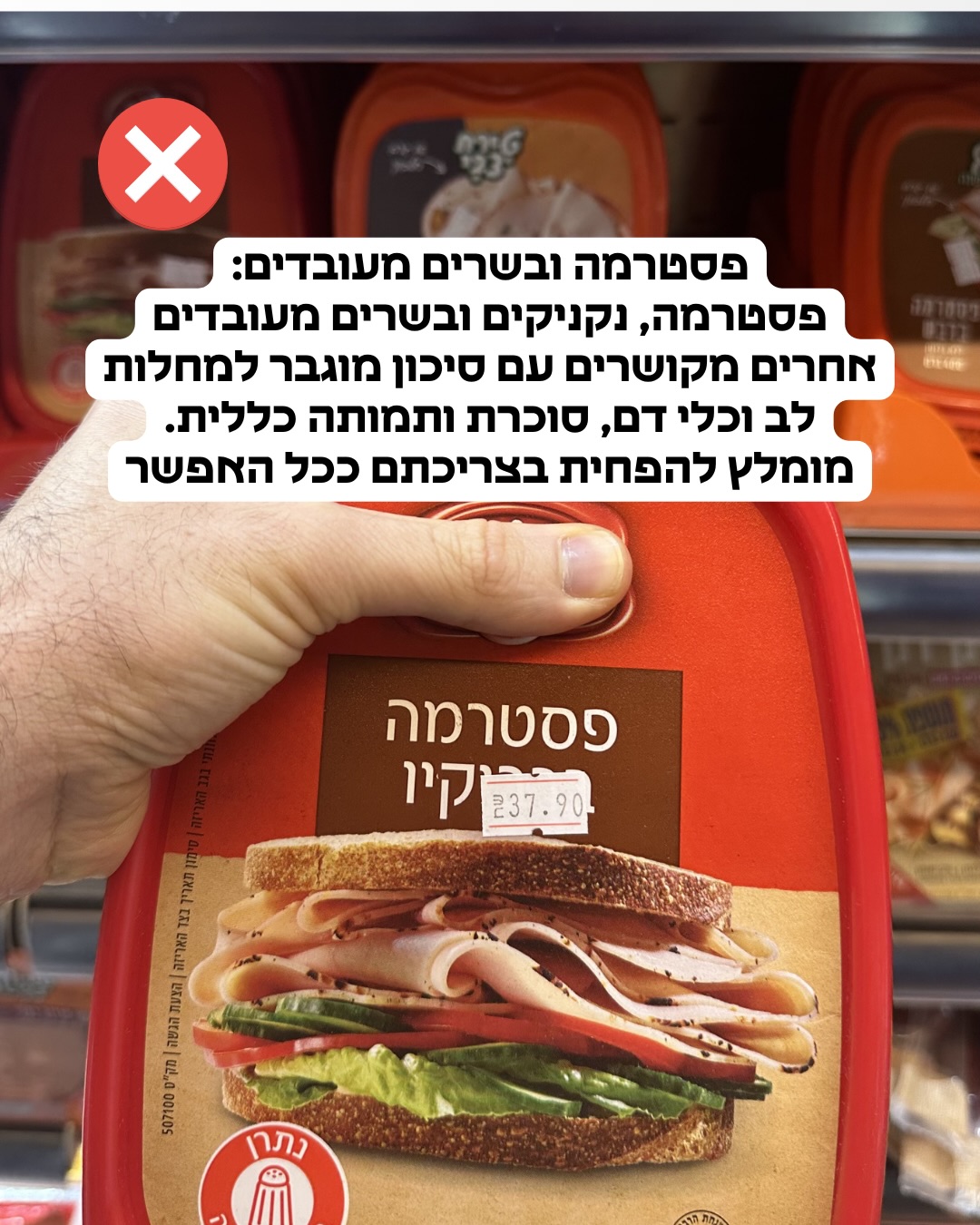
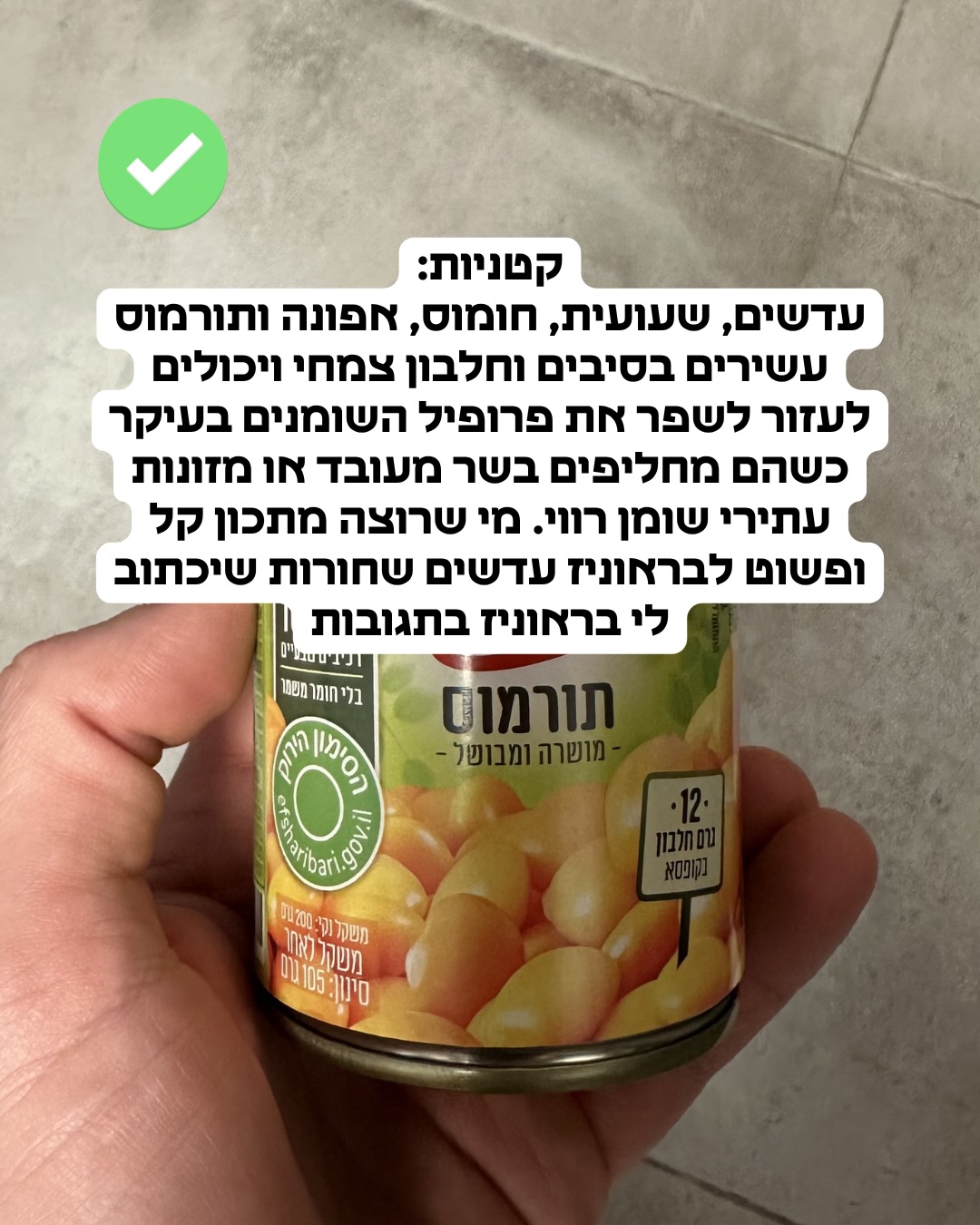
"צריכת בשרים מעובדים קשורה לסיכון מוגבר למחלות לב וכלי דם ולסוכרת, ולכן מומלץ להפחית בצריכתם."
מסקנת הבדיקה:
קיימות ראיות עקביות במחקרים אפידמיולוגיים ומטה-אנליזות לכך שצריכת בשר מעובד קשורה לסיכון מוגבר למחלות לב וכלי דם ולסוכרת מסוג 2, וארגוני בריאות ממליצים להגביל את צריכתו. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Red meat consumption, cardiovascular diseases, and diabetes: a systematic review and meta-analysis.
Observational studies show inconsistent associations of red meat consumption with cardiovascular disease (CVD) and diabetes. Moreover, red meat consumption varies by sex and setting, however, whether the associations vary by sex and setting remains unclear. This systematic review and meta-analysis was conducted to summarize the evidence concerning the associations of unprocessed and processed red meat consumption with CVD and its subtypes [coronary heart disease (CHD), stroke, and heart failure], type two diabetes mellitus (T2DM), and gestational diabetes mellitus (GDM) and to assess differences by sex and setting (western vs. eastern, categorized based on dietary pattern and geographic region). Two researchers independently screened studies from PubMed, Web of Science, Embase, and the Cochrane Library for observational studies and randomized controlled trials (RCTs) published by 30 June 2022. Forty-three observational studies (N = 4 462 810, 61.7% women) for CVD and 27 observational studies (N = 1 760 774, 64.4% women) for diabetes were included. Red meat consumption was positively associated with CVD [hazard ratio (HR) 1.11, 95% confidence interval (CI) 1.05 to 1.16 for unprocessed red meat (per 100 g/day increment); 1.26, 95% CI 1.18 to 1.35 for processed red meat (per 50 g/day increment)], CVD subtypes, T2DM, and GDM. The associations with stroke and T2DM were higher in western settings, with no difference by sex. Unprocessed and processed red meat consumption are both associated with higher risk of CVD, CVD subtypes, and diabetes, with a stronger association in western settings but no sex difference. Better understanding of the mechanisms is needed to facilitate improving cardiometabolic and planetary health.…
PMID: 37264855
-
link
Estimated effects of reductions in processed meat consumption and unprocessed red meat consumption on occurrences of type 2 diabetes, cardiovascular disease, colorectal cancer, and mortality in the USA: a microsimulation study.
High consumption of processed meat and unprocessed red meat is associated with increased risk of multiple chronic diseases, although there is substantial uncertainty regarding the relationship for unprocessed red meat. We developed a microsimulation model to estimate how reductions in processed meat and unprocessed red meat consumption could affect rates of type 2 diabetes, cardiovascular disease, colorectal cancer, and mortality in the US adult population. We used data from two versions of the US National Health and Nutrition Examination Survey, one conducted during 2015-16 and one conducted during 2017-18, to create a simulated US population. The starting cohort was restricted to respondents aged 18 years or older who were not pregnant and had 2 days of dietary-recall data. First, we used previously developed risk models to estimate the baseline disease risk of an individual. For type 2 diabetes we used a logistic-regression model and for cardiovascular disease and colorectal cancer we used Cox proportional-hazard models. We then multiplied baseline risk by relative risk associated with individual processed meat and unprocessed red meat consumption. Prevented occurrences of type 2 diabetes, cardiovascular disease, colorectal cancer, and mortality were computed by taking the difference between the incidence in the baseline and intervention scenarios. All stages were repeated for ten iterations to correspond to a 10-year time span. Scenarios were reductions of 5%, 10%, 30%, 50%, 75%, and 100% in grams consumed of processed meat, unprocessed red meat, or both. Each scenario was repeated 50 times for uncertainty analysis. The total number of individual respondents included in the simulated population was 8665, representing 242 021 876 US adults. 4493 (51·9%) of 8665 individuals were female and 4172 (48·1%) were male; mean age was 49·54 years (SD 18·38). At baseline, weighted mean daily consumption of processed meat was 29·1 g, with a 30% reduction being 8·7 g per day, and of unprocessed red meat was 46·7 g, with a 30% reduction being 14·0 g per day. We estimated that a 30% reduction in processed meat intake alone could lead to 352 900 (95% uncertainty interval 345 500-359 900) fewer occurrences of type 2 diabetes, 92 500 (85 600-99 900) fewer occurrences of cardiovascular disease, 53 300 (51 400-55 000) fewer occurrences of colorectal cancer, and 16 700 (15 300-17 700) fewer all-cause deaths during the 10-year period. A 30% reduction in unprocessed red meat intake alone could lead to 732 600 (725 700-740 400) fewer occurrences of type 2 diabetes, 291 500 (283 900-298 800) fewer occurrences of cardiovascular disease, 32 200 (31 500-32 700) fewer occurrences of colorectal cancer, and 46 100 (45 300-47 200) fewer all-cause deaths during the 10-year period. A 30% reduction in both processed meat and unprocessed red meat intake could lead to 1 073 400 (1 060 100-1 084 700) fewer occurrences of type 2 diabetes, 382 400 (372 100-391 000) fewer occurrences of cardiovascular disease, 84 400 (82 100-86 200) fewer occurrences of colorectal cancer, and 62 200 (60 600-64 400) fewer all-cause deaths during the 10-year period. Reductions in processed meat consumption could reduce the burden of some chronic diseases in the USA. However, more research is needed to increase certainty in the estimated effects of reducing unprocessed red meat consumption. The Wellcome Trust.…
PMID: 38969472
-
link
Potential health hazards of eating red meat.
Red meat (beef, veal, pork, lamb and mutton) consumption contributes several important nutrients to the diet, for example essential amino acids, vitamins (including B12) and minerals (including iron and zinc). Processed red meat (ham, sausages, bacon, frankfurters, salami, etc.) undergoes treatment (curing, smoking, salting or the use of chemical preservatives and additives) to improve its shelf life and/or taste. During recent decades, consumption of red meat has been increasing globally, especially in developing countries. At the same time, there has been growing evidence that high consumption of red meat, especially of processed meat, may be associated with an increased risk of several major chronic diseases. Here, a comprehensive summary is provided of the accumulated evidence based on prospective cohort studies regarding the potential adverse health effects of red meat consumption on major chronic diseases, such as diabetes, coronary heart disease, heart failure, stroke and cancer at several sites, and mortality. Risk estimates from pooled analyses and meta-analyses are presented together with recently published findings. Based on at least six cohorts, summary results for the consumption of unprocessed red meat of 100 g day…
PMID: 27597529
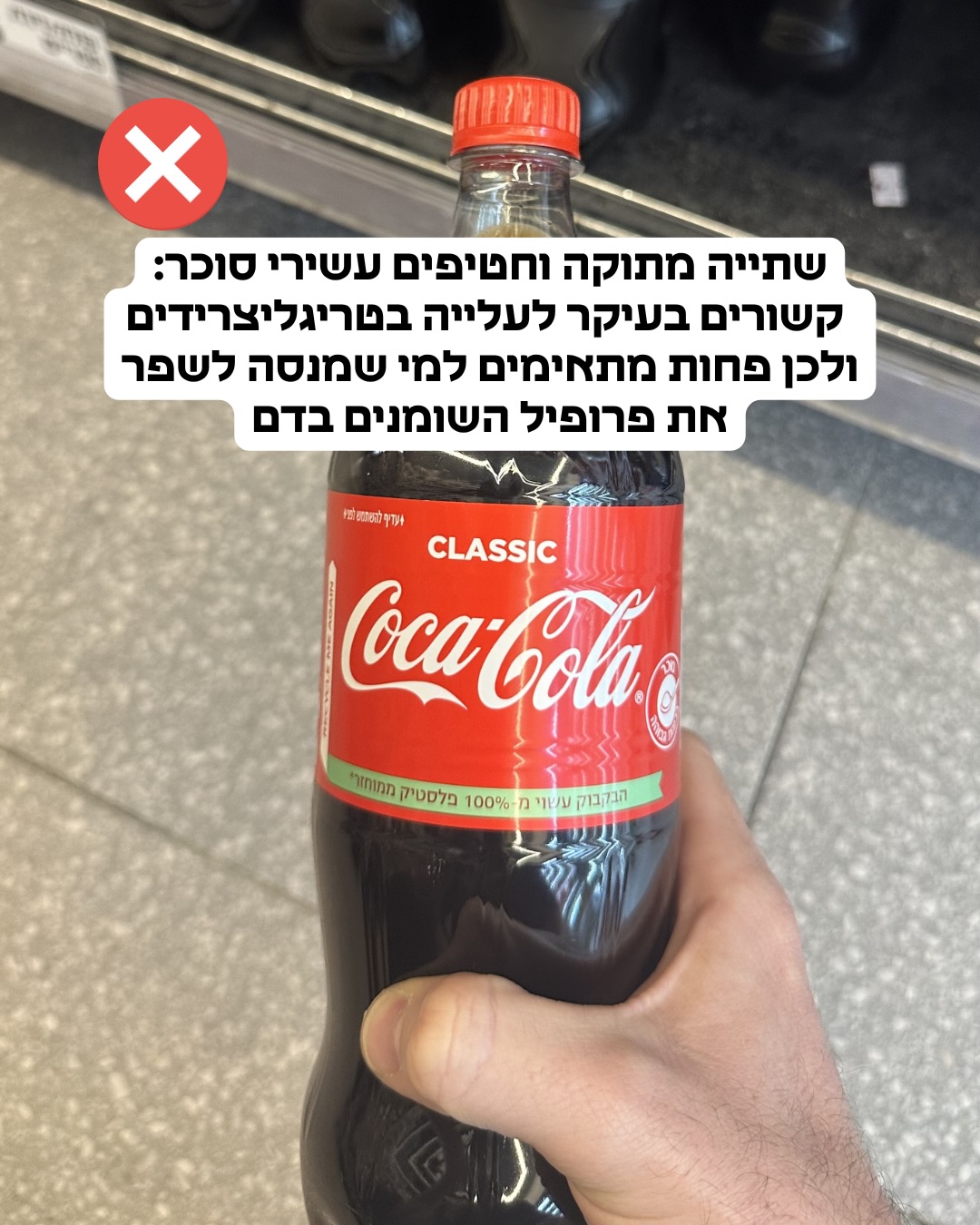
"צריכת אלכוהול ומשקאות עתירי סוכר קשורה לעלייה ברמות הטריגליצרידים בדם, ולכן הפחתתם עשויה לשפר את פרופיל השומנים."
מסקנת הבדיקה:
צריכה מופרזת של אלכוהול ומשקאות ממותקים בסוכר מזוהה בספרות המדעית כגורם התורם לעלייה ברמות הטריגליצרידים בדם, והפחתתם נחשבת לאסטרטגיה תזונתית לשיפור פרופיל השומנים. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Association between healthy beverage index and kidney and cardiovascular risk factors in patients with type 2 diabetes: a cross-sectional study in Iran.
<h4>Background</h4>Limited studies have addressed the overall quality of beverages in participants with type 2 diabetes. Therefore, this study aimed to examine the relationship between a healthy beverage index (HBI) and risk factors of kidney and cardiovascular disease in patients with type 2 diabetes.<h4>Methods</h4>This comparative cross-sectional study was conducted on 245 Iranian with type 2 diabetes. A FFQ with 168 items was used to assess dietary intakes. Participants were categorized into three groups based on the HBI. The association between the HBI with the investigated variables was assessed by binary logistic regression that adjusted for age, total calorie intake, body mass index (BMI), physical activity, smoking, using blood sugar-lowering pills, marital status, occupation, economic status, and education level.<h4>Results</h4>After adjusting for confounders, our findings showed a significant inverse relationship between the HBI and urine albumin (odds ratio (OR): 0.91, 95% CI: (0.73 to 0.98)), and urine creatinine (OR: 0.85, 95% CI: (0.73 to 0.99)); as well as total cholesterol (OR: 0.93, 95% CI: (0.87 to 1.00)), diastolic blood pressure (OR: 0.94, 95% CI: (0.89 to 1.00)), and two-hour blood sugar (OR: 0.94, 95% CI: (0.89 to 1.00)).<h4>Conclusion</h4>The current study clarifies that a healthy beverage index may be associated with urine albumin, urine creatinine, total cholesterol, diastolic blood pressure, and two-hour blood sugar. The healthy beverage index warrants further consideration in relation to risk factors for kidney disease, lipid profile, and blood pressure among individuals with type 2 diabetes.…
PMID: 40993803
-
link
Causal Relationship Between 38 Dietary Factors, Including Sugar and Alcohol Intakes, and Polycystic Ovary Syndrome: A Two-Sample Mendelian Randomization Study.
<h4>Purpose</h4>Emerging evidence suggests that diets high in sugar consumption may be implicated in the development of polycystic ovary syndrome (PCOS), but the causal nature of these associations remains unclear. This study aimed to explore the potential causal links between 38 specific dietary factors (including alcohol and added sugar), particularly sugar-sweetened beverage intake, and the risk of PCOS.<h4>Patients and methods</h4>A two-sample Mendelian randomization (MR) approach was employed using genome-wide association study summary statistics. The inverse-variance weighted (IVW) method served as the primary analytical tool, with supplementary assessments conducted using the weighted median, weighted mode, and MR-Egger regression methods. Cochran's Q test evaluated heterogeneity, while MR-Egger regression and MR pleiotropy residual sum and outlier (MR-PRESSO) analysis were applied to detect horizontal pleiotropy. Robustness of findings was further assessed through leave-one-out analysis, along with visualization via forest and funnel plots.<h4>Results</h4>The IVW analysis indicated potential causal associations between PCOS and alcohol intake frequency (OR = 1.39, 95% CI: 1.03-1.88, P = 0.03) and sugar added to tea (OR = 0.43, 95% CI: 0.21-0.89, P = 0.022); these associations were only supported by the IVW method and not by the other MR methods. No significant associations were observed for the 36 other dietary factors. For all 38 dietary factors, the sensitivity analyses confirmed that the results were not driven by individual instrumental variables, no significant heterogeneity was observed using Cochran's Q test, and MR-Egger regression and MR-PRESSO detected no evidence of horizontal pleiotropy or outliers.<h4>Conclusion</h4>Genetically predicted alcohol intake frequency was causally associated with PCOS. Although the initial hypothesis considered added sugar as a potential risk factor, the observed protective association of "sugar in tea" could reflect a proxy effect of tea consumption itself rather than a direct benefit of sugar. Further population-based studies are warranted for validation.…
PMID: 42022860
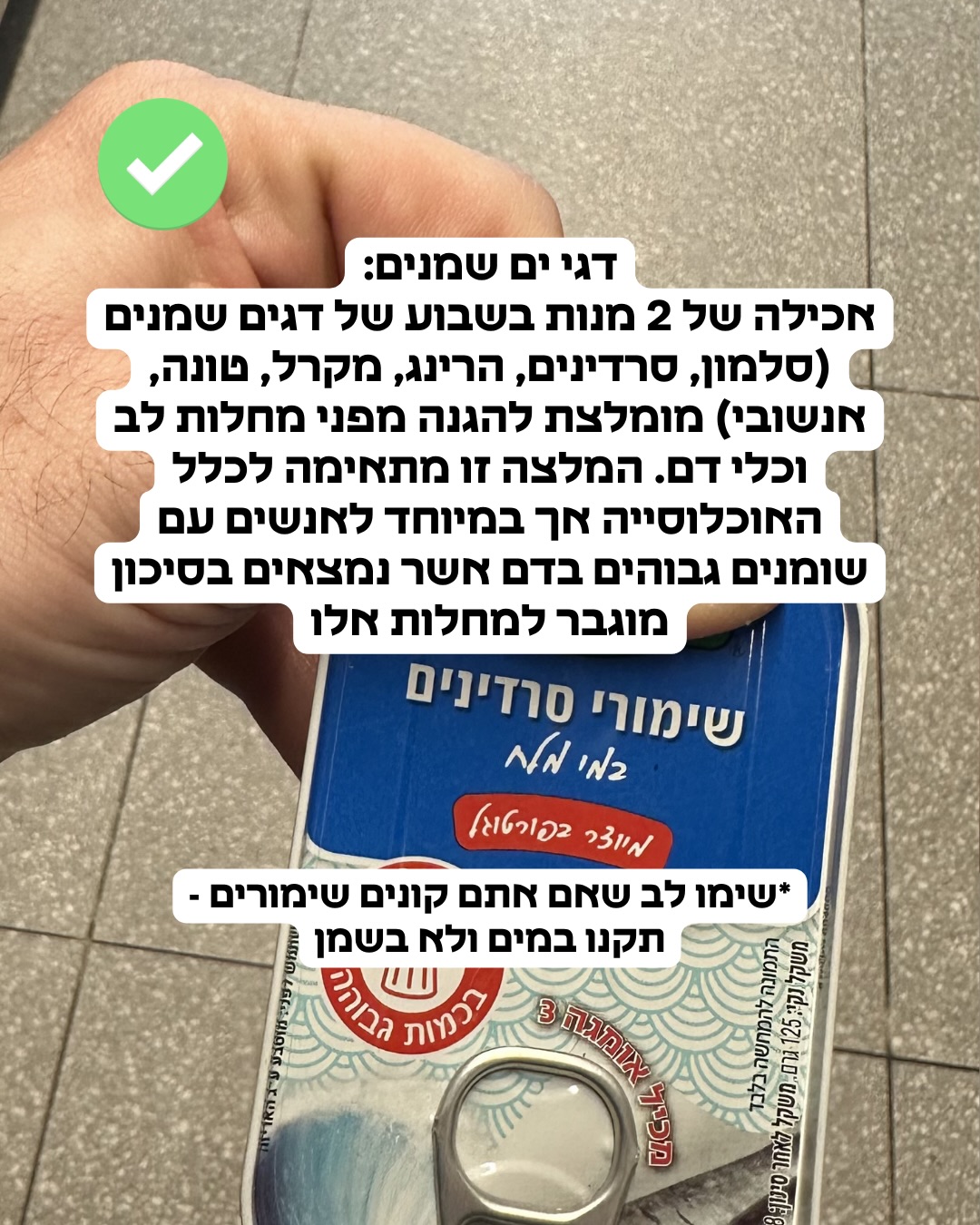
"אכילת שתי מנות של דגים שמנים בשבוע (כגון סלמון, סרדינים או מקרל) מומלצת להגנה מפני מחלות לב וכלי דם."
מסקנת הבדיקה:
המלצות תזונתיות רבות מבוססות על מחקרים המצביעים על כך שצריכת דגים שמנים העשירים באומגה 3 מסייעת בהגנה מפני מחלות לב וכלי דם, אם כי קיימים דיונים מדעיים על עוצמת ההשפעה של תוספים לעומת צריכה מהמזון. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Omega-3 and omega-6 polyunsaturated fatty acids: Dietary sources, metabolism, and significance - A review.
Linoleic acid (LA) (n-6) and α-linolenic acid (ALA) (n-3) are essential fatty acids (EFAs) as they cannot be synthesized by humans or other higher animals. In the human body, these fatty acids (FAs) give rise to arachidonic acid (ARA, n-6), eicosapentaenoic acid (EPA, n-3), and docosahexaenoic acid (DHA, n-3) that play key roles in regulating body homeostasis. Locally acting bioactive signaling lipids called eicosanoids derived from these FAs also regulate diverse homeostatic processes. In general, ARA gives rise to pro-inflammatory eicosanoids whereas EPA and DHA give rise to anti-inflammatory eicosanoids. Thus, a proportionally higher consumption of n-3 PUFAs can protect us against inflammatory diseases, cancer, cardiovascular diseases, and other chronic diseases. The present review summarizes major sources, intake, and global consumption of n-3 and n-6 PUFAs. Their metabolism to biosynthesize long-chain PUFAs and eicosanoids and their roles in brain metabolism, cardiovascular disease, obesity, cancer, and bone health are also discussed.…
PMID: 29715470
-
link
Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease.
Researchers have suggested that omega-3 polyunsaturated fatty acids from oily fish (long-chain omega-3 (LCn3), including eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)), as well as from plants (alpha-linolenic acid (ALA)) benefit cardiovascular health. Guidelines recommend increasing omega-3-rich foods, and sometimes supplementation, but recent trials have not confirmed this. To assess effects of increased intake of fish- and plant-based omega-3 for all-cause mortality, cardiovascular (CVD) events, adiposity and lipids. We searched CENTRAL, MEDLINE and Embase to April 2017, plus ClinicalTrials.gov and World Health Organization International Clinical Trials Registry to September 2016, with no language restrictions. We handsearched systematic review references and bibliographies and contacted authors. We included randomised controlled trials (RCTs) that lasted at least 12 months and compared supplementation and/or advice to increase LCn3 or ALA intake versus usual or lower intake. Two review authors independently assessed studies for inclusion, extracted data and assessed validity. We performed separate random-effects meta-analysis for ALA and LCn3 interventions, and assessed dose-response relationships through meta-regression. We included 79 RCTs (112,059 participants) in this review update and found that 25 were at low summary risk of bias. Trials were of 12 to 72 months' duration and included adults at varying cardiovascular risk, mainly in high-income countries. Most studies assessed LCn3 supplementation with capsules, but some used LCn3- or ALA-rich or enriched foods or dietary advice compared to placebo or usual diet.Meta-analysis and sensitivity analyses suggested little or no effect of increasing LCn3 on all-cause mortality (RR 0.98, 95% CI 0.90 to 1.03, 92,653 participants; 8189 deaths in 39 trials, high-quality evidence), cardiovascular mortality (RR 0.95, 95% CI 0.87 to 1.03, 67,772 participants; 4544 CVD deaths in 25 RCTs), cardiovascular events (RR 0.99, 95% CI 0.94 to 1.04, 90,378 participants; 14,737 people experienced events in 38 trials, high-quality evidence), coronary heart disease (CHD) mortality (RR 0.93, 95% CI 0.79 to 1.09, 73,491 participants; 1596 CHD deaths in 21 RCTs), stroke (RR 1.06, 95% CI 0.96 to 1.16, 89,358 participants; 1822 strokes in 28 trials) or arrhythmia (RR 0.97, 95% CI 0.90 to 1.05, 53,796 participants; 3788 people experienced arrhythmia in 28 RCTs). There was a suggestion that LCn3 reduced CHD events (RR 0.93, 95% CI 0.88 to 0.97, 84,301 participants; 5469 people experienced CHD events in 28 RCTs); however, this was not maintained in sensitivity analyses - LCn3 probably makes little or no difference to CHD event risk. All evidence was of moderate GRADE quality, except as noted.Increasing ALA intake probably makes little or no difference to all-cause mortality (RR 1.01, 95% CI 0.84 to 1.20, 19,327 participants; 459 deaths, 5 RCTs),cardiovascular mortality (RR 0.96, 95% CI 0.74 to 1.25, 18,619 participants; 219 cardiovascular deaths, 4 RCTs), and it may make little or no difference to CHD events (RR 1.00, 95% CI 0.80 to 1.22, 19,061 participants, 397 CHD events, 4 RCTs, low-quality evidence). However, increased ALA may slightly reduce risk of cardiovascular events (from 4.8% to 4.7%, RR 0.95, 95% CI 0.83 to 1.07, 19,327 participants; 884 CVD events, 5 RCTs, low-quality evidence), and probably reduces risk of CHD mortality (1.1% to 1.0%, RR 0.95, 95% CI 0.72 to 1.26, 18,353 participants; 193 CHD deaths, 3 RCTs), and arrhythmia (3.3% to 2.6%, RR 0.79, 95% CI 0.57 to 1.10, 4,837 participants; 141 events, 1 RCT). Effects on stroke are unclear.Sensitivity analysis retaining only trials at low summary risk of bias moved effect sizes towards the null (RR 1.0) for all LCn3 primary outcomes except arrhythmias, but for most ALA outcomes, effect sizes moved to suggest protection. LCn3 funnel plots suggested that adding in missing studies/results would move effect sizes towards null for most primary outcomes. There were no dose or duration effects in subgrouping or meta-regression.There was no evidence that increasing LCn3 or ALA altered serious adverse events, adiposity or lipids, although LCn3 slightly reduced triglycerides and increased HDL. ALA probably reduces HDL (high- or moderate-quality evidence). This is the most extensive systematic assessment of effects of omega-3 fats on cardiovascular health to date. Moderate- and high-quality evidence suggests that increasing EPA and DHA has little or no effect on mortality or cardiovascular health (evidence mainly from supplement trials). Previous suggestions of benefits from EPA and DHA supplements appear to spring from trials with higher risk of bias. Low-quality evidence suggests ALA may slightly reduce CVD event risk, CHD mortality and arrhythmia.…
PMID: 30019766
-
link
Omega-3 fatty acids and cardiovascular disease.
Cardioceuticals are nutritional supplements that contain all the essential nutrients including vitamins, minerals, omega-3-fatty acids and other antioxidants like a-lipoic acid and coenzyme Q10 in the right proportion that provide all round protection to the heart by reducing the most common risks associated with the cardiovascular disease including high low-density lipoprotein cholesterol and triglyceride levels and factors that contribute to coagulation of blood. Omega-3 fatty acids have been shown to significantly reduce the risk for sudden death caused by cardiac arrhythmias and all-cause mortality in patients with known coronary heart disease. Omega-3 fatty acids are also used to treat hyperlipidemia and hypertension. There are no significant drug interactions with omega-3 fatty acids. The American Heart Association recommends consumption of two servings of fish per week for persons with no history of coronary heart disease and at least one serving of fish daily for those with known coronary heart disease. Approximately 1 g/day of eicosapentaenoic acid plus docosahexaenoic acid is recommended for cardio protection. Higher dosages of omega-3 fatty acids are required to reduce elevated triglyceride levels (2-4 g/day). Modest decreases in blood pressure occur with significantly higher dosages of omega-3 fatty acids.…
PMID: 25720716

ד״ר אסי שגיב
דירוג זה מבוסס על 5 דוחות אימות קודמים.








האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.